In my last post, published last week, I made a collection with the most interesting definitions of “Internet of things” or this “connected world” accesible for everyone without discrimination because of economic, social or functional diversity reasons.
At the sprint by connect everything and everyone, in the disability world, the called: “connected home” and orientation and mobility are de winner. These two aspects make life easier to people with disabilities.
In the framework of the “connected home”, the options of applying Internet of Things in the improvement of the quality of life are very spacious. Here, there are some examples:
• Philips Hue lighting system eases the communication between people with hearing disabilities, using lights to notify the person different signs and sound warnings that they may not listen. This system provides an open software platform, which facilitates its use from external applications adapted to each user.
• Brands such as Miele and Bosh announced the inclusion of intelligence and connection with smartphones in their appliances, both for the same control to offer other types of services (recipes, shopping list). Control of electrical appliances to drive, even voice, can be a big advantage for people with motor difficulties, because the use of the conventional controls could be a problem for them.
• The project SANDS(CARTIF) offers the possibility of the electrical appliances to adapt to the tastes of users automatically. Users only have to express their opinion. Appliances from users with similar profiles, communicate with each other to share recipes that are combined by the machine itself according to each user. SANDS, as in the previous case, allows the configuration and commissioning of electrical appliances from a network application. Automatic adaptation of the recipes could help people with memory problems, or cognitive disabilities to use appliances according to your tastes without having extensive knowledge of the commands.
To facilitate mobility and orientationwe have projects such as:
• AT&T and Permobil wheelchair, with wireless. Users share information about their status and situation through a secure cloud. You can also modify aspects like the position of the chair.
• A “Search for parking” systems, as the Viarium Technology, provides information to people with disabilities related to parking.
• Danok of Konectik is an application that uses iBeacon sensors and technology to provide information about the environment. This application is especially useful for blind people and people with cognitive disabilities.
• The Aditium Kango project, using cards NFC for tracking schoolchildren during their route to school. This project can also be useful for older people and people with cognitive disabilities or mental illness.
• The connected headset, Oticon Opn, uses Wi-Fi connectivity and recipes based on TWITTERFEED (IF This Then That) in addition to the traditional functionality, to allow deaf people can set it up to receive alerts such as a bell, or the activation of a smoke detector.
In short, we can see that road to “interconnection of all” can be closer thanks to advances in the IoT.
Nikola Tesla was a visionary engineer and physical of the 19th century. He devoted much of his life to wireless energy transmission, as have done with radio. He was the first that imagined a connected world which he described with these words: “Anyone, at sea or earth, could receive news or particular messages from anywhere in the world, with a simple and inexpensive device in your pocket; the Earth would seem to an immeasurable brain, capable of emitting a response from anywhere”.
The now called Internet of Things (IoT) is not a big step toward “immeasurable brain”? For those who are dedicated to new technologies, should we be motivated in order to not excluding anyone from this connected world, either for economic, social or functional diversity reasons?
“Internet of Things” is an expression that today has many descriptions, but we can say that is a term invented in 1999 by Kevin Asthon, co-founder of MIT and creator of a global standard system to RFID and others sensors. He used the IoT term to describe a system where Internet is connected to the physical world through ubiquitous sensors.
One of the most formal descriptions belongs to Cluster of European Research Projects (IERC, 2009): “Internet of Things (IOT) is an integrated part of Future Internet and could be defined as a dynamic global network infrastructure with self-configuring capabilities based on standard and interoperable communication protocols where physical and virtual “things” have identities, physical attributes, virtual personalities and use intelligent interfaces, and are seamlessly integrated into the information network”.
Recently, Diego Soriano (CENTAC) described IoT concept in a more friendly way: “IoT is the technology that allows using joint, simple and cheap form, many electronics elements connected to the Internet”
If we combine these ideas with these technological aspects: • The large number of available sensors and wearables and in design phase. • The use of technologies such as Big Data and Cloud, to analyze, management and store generated data by these devices.
IoT provide enough elements to create products and systems capable of making our lives easier. They are able to interact with the world around us without having to connect to it via cables (alerts in our smartphones, tablet or bracelet from others devices, ability to interact with appliances and security elements in our home from a different location, …). As we will see below this “make our lives easier”, IoT can be especially useful and meaningful for people with disabilities and can imply an advance in their independence.
On the one hand, the general products existence provides application in different fields to different collectives, and, on the other hand, we have specific solutions for disabilities people that, as we always say, they will evolve by quality life to everyone. Compare it with the evolution of accessible architecture.
The following week, we will go on analyzing the different applicances of IoT in the dissability world. In addition of the “connected home”, we will see some specific examples which are already in the market.
We are used to see how new technologies help people with physical disabilities: automatic wheel chairs, revolutionary prosthesis and even image or voice sensors directly connected to the brain through electrodes. But what about people with a mental disability? Let’s think on those persons that suffer schizophrenia. This is a chronic condition characterized by certain behaviors that are abnormal for the community. In particular, many people with schizophrenia have difficulty recognizing emotions in the facial expressions of other people, which seriously affects social behavior. Furthermore, this difficulty is not limited to schizophrenia, but is also observed in cases of mania, dementia, brain damage, autism etc.
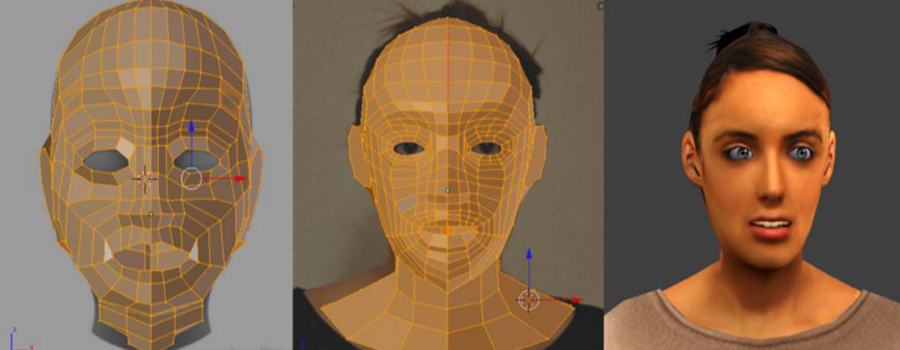
Here come into play social robotics technologies. A social robot is a robot that interacts and communicates with people (or other robots) following social behaviors and rules. Furthermore, traditionally a robot is assumed to be materialized in the form of physical device. However, the same interaction skills designed for a physical robot can be integrated into a virtual character represented in a computer. From this viewpoint, an Avatar may be considered to be a robot, in line with the new technological paradigm in which the boundary between the physical and the virtual reality is progressively diluted.
Now, what advantages does the use of Avatars in psychological and psychiatric therapies have? In my opinion, these advantages are innumerable. An avatar can reach an expressiveness level comparable (if not superior) to that of a physical robot, and even a real personal. Not even a hyper-realistic human appearance is needed: a simple cartoon can be extremely expressive. (Let’s think of the coyote when, in pursuit of the roadrunner, exceeds the limit of the cliff). In addition, unlike a real person, the expressiveness of an avatar can be controlled to the millimeter by a therapist. This way, the virtual avatar can display emotions in varying degrees, from emerging to very marked, randomly or in progression, even depending on the user behavior.
Another great aspect involved is sensorization. Here, the Computer Vision technologies play a decisive role. We are used to our mobile phone camera that detects and tracks faces, identifies which faces correspond to people in our family or social environment and determine when they open their eyes and smile. Obviously, this technology can be put at the service of perceiving the user’s attitude during interaction: whether the user smiles or is sad, if he/she is calm or nervous or feels anxious. In addition, certainly voice analysis can supplement this information. The words used by the person say a lot about his/her mood. In addition, the tone and rhythm also provide crucial information: an angry person talks fast and loud, while someone who is bored speaks slowly, in a slurred speech. Certainly, nowadays the voice analysis goes a step behind the image analysis, probably because it is very close to artificial intelligence that still represents a challenge (although increasingly affordable by technology).
Where does this lead us?To a virtual (or physical) avatar that tracks the user’s face with its eyes, interprets user emotions and reacts accordingly to them, talk friendly and can be supervised by a therapist, with the advantage of being available 24 hours day. A companion, ultimately, that serves as a personal trainer to improve the perception of human emotions. This is not the future. This is the present.
VideoGames, social networks and wearables have been installed in our lives since a few years. They occupy much of our free time, allowing new methods of interacting with families and friends. They are part of the so called Information and Communication Technologies (ICTs), a pillar of the new concept of health eHealth that gives meaning to the use of social networks, videogames and wearables in order to improve the quality of life of the people.
The World Health Organization (WHO) defines eHealth as “the use of information and communication technologies for better health monitoring; for example, for the treatment of certain patients, promote research, create tools for education students, do screaning in various diseases”. The main participants of the eHealth, patients (ePatient) and doctors (eDoctor) are aware of that technology can improve the performance of health systems and make use of it for their benefit.
The objective of eHealth is to focus the health system on the specific needs of citizens by providing and exchanging information. Hence patients, professionals and health managersprovide knowledge to the care chain with the aim of promoting the prevention, diagnosis early and specialized treatment.
The main services that provide e-health are telemedicine, telecare, online consultations, telematic management, monitoring and treatment delivery and management big data the health management entails. Professionals, patients and managers are closer, easing efforts, avoiding displacements and reducing resources while improving service.
The new technologies, social networks, specialized blogs, wikis, podcasts, videos and messaging services, video games, wearables, of whom know their lucid and social part allow the exchange of information and knowledge, basic aspect in e-health, through:
Patients’ Communities in whom share experiences, talk about their disease, treatments and resources available. Patients have company.
Professionals’ Communities to share experiences, knowledge, approaches, concerns, views, etc.
Health networks that connect patients with professionals, and provide useful information to users. They often include valuation services, testimonials, advice, recommendations, etc.
Health information Sources available to patients and professionals who report on the latest developments and report on the health aspect.
Direct communication through the latest technologies (videoconferencing, chat, blogs, forums, etc.) that enable remote assistance, and allow the patient and the professional maintain a close relationship.
Patient monitoring and treatment, application usage and wearables devices that allow continuous monitoring of the health conditions of patients, especially chronic, and evaluate, motivate and guide their treatment.
Treatments and health monitoring of chronic patients require monitoring professionals who perform the testing and evaluation of patients. So far, it requires the need to go to the health center and make an appointment with the appropriate professionals. Mobile applications, wearables and video games allow the patient can perform their own testsat home providing professional data necessary to carry out the necessary assessments without resorting to consultation, reducing costs, increasing the rate of monitoring and increased adherence to treatment.
There are a lot of applications related to eHealth and especially chronic patients such as diabetes. Videogames, or Serious Games, as they are called, are a kind of applications that go beyond entertainment and allow motivate, evaluate and inform patients, allow greater adherence to treatment in patients. These applications and devices can increase patient knowledge about their disease and enhance training and skills development and extraction of valuable information for professionals, while fun and involves the patient.
It is clear that eHealth offers many advantages but, are they accessible to everyone? The basis of eHealth is ICT and therefore requires knowledge and assimilation of them. Not everybody dominate these technologies. The elderly have greater difficulty in accessing Internet so that, there is a handicap to overcome in order to they can be part of eHealth. They also tend to have misgivings about changes and prefer not to change.
As you can read, eHealth facilitates the exchange of knowledge, treatment adherence reducing costs and increasing the knowledge of patients and professionals. But its implementation is slow because it depends not only on technology but the attitude of people to them.
The increase in life expectancy, coupled with the decline in the birth rate results in an increasingly aging population. According to projections by the National Statistics Institute, 30% of the population will be aged over 65 in 2050, and of these a third will be octogenarians.
This large population will present assistance needs which will scarcely be covered by the working population. Assistive robotics has emerged as a solution that can help alleviate this problem. Assistive robotics is the area of service robotics in which the robot interacts directly with the individual. The scope is very broad; robots can be designed to aid a person’s mobility (standing, walking, etc.), help in physical or cognitive rehabilitation and supply social support, care and entertainment. Unfortunately, the expectations that have been generated for this type of robots have been very high, partly because of movie robots: Walle, R2D2, C3PO, Short Circuit, etc., all have capabilities similar to humans. However, there are few robots that have been introduced in the market except for robot vacuum cleaners, lawn mowers and pool cleaners. The success of these robots is undoubtedly that they carry out very specific activities at a reasonable cost.
The main difficulty with care robotics is that they interact with people, so they must have robust perceptual systems, motion, manipulation, cognition capacities and interaction systems designed to communicate with humans using natural and gestural language.
The state of the current technology does not allow robots with those capabilities of movie robots to be developed. The solution is to develop robots with capacities restricted to defined contexts, limiting its functionality while ensuring proper integration of all subsystems that can overcome the envisaged situations. For example, the solution of a sequential complex problem such as a verbal dialogue with a robot can be to restrict the vocabulary and the topic discourse. This contextual grouping can be applied to other aspects like visual recognition or emotional control.
Another recommendation is that experimentation needs to be done from the beginning in real environments where the robot must work. Often, the efforts are focused on developments in the laboratory away from the end users and services to be provided.
A good methodology is to do iterative and successive refinements in the robot, incorporating new features and capabilities over time. The definition of metrics allows robot evolution and performance to be measured according to user requirements.
However, not only scientific barriers prevent robots from reaching the market. There are also social barriers that must be overcome. Often, there are serious drawbacks which prevent robots from being accepted by people: appearance, fear of technology, or fear of losing their job to the robots. These social aspects should be considered in the early stages of robot design.
Over the last few years in CARTIF, we have applied this design methodology based on user needs. Our latest challenge is Sacarino, a robot with social and interaction abilities which will provide therapy, assistance and entertainment in one of the living units at the Hermanas Hospitalarias Hospital in Palencia. Hopefully, we shall be able to contribute to the development of welfare robots and, in a few years’ time, care robotics will be a reality which could provide value-added services and would be present in our homes and hospitals.
This is E2REBOT, our neurorehabilitation robot which enables and makes easier the rehabilitation of the upper limbs of people with some kind of neuromotor disability.