In a first approach to the world of Augmented Reality, we established the differences between technologies of mixed, augmented and virtual reality. In this second installment, we are going to review the applications that are already being made of these realities in the health sector.
Medical data visualization
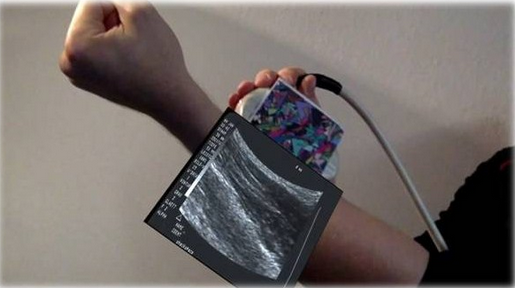
Applications aiming at the agile viewing of patient data such as ultrasound, tomography images … obtaining a more accurate view of data improving diagnoses and facilitating the decision making for possible surgical interventions.
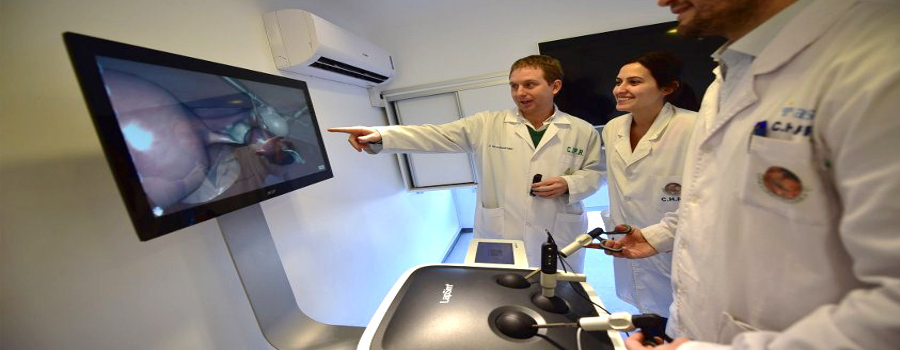
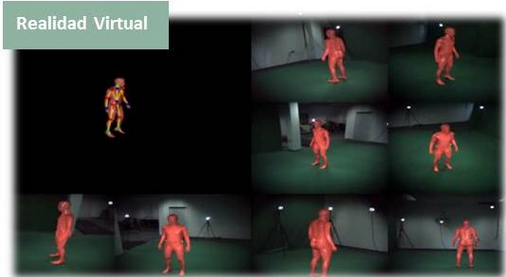
RV does not need the human patient to be present, since it deals more with off-line simulation. This makes it very suitable for training.
The simulator called LapSim emulates a real surgery with the laparoscopic technique using a haptic device that allows reproducing the sensations of the realized movements.
Surgery
Both AR and VR are able to improve the surgery by allowing the preparation of them with patient data and testing various techniques to choose the most convenient. At the same time, it is able to guide and mark relevant information during the development of the surgery obtaining more efficient and less invasive surgeries.
MEVIS system allows to prepare the surgery using 3D images of x-rays and tomographies to reconstruct the locations of blood vessels. In addition, during the development of them, is able to register the planning data and display blood vessels in different colours.
Diagnosis, therapy and rehabilitation
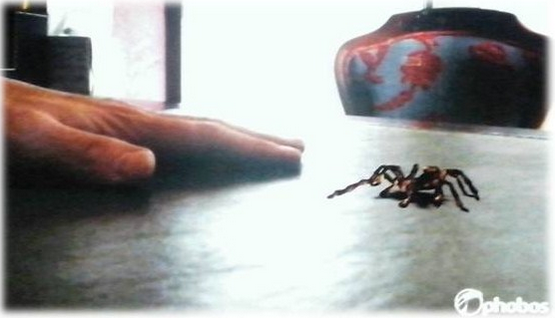
The AR and VR have a clear application in tests for diagnosis of diseases, treatment of phobias and support and incentive in the rehabilitation generating virtual and safe situations
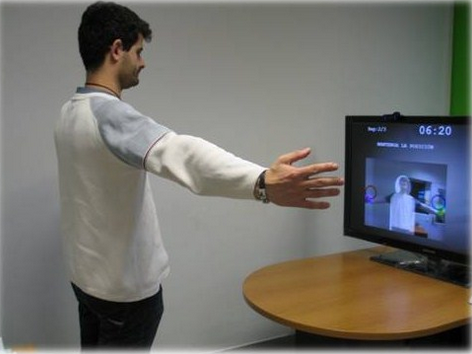
Rehabilitation system for the health platform Tratamiento 2.0 by CARTIF. The system allows managing rehabilitation exercises for the patients by the health personnel and the patients perform the exercises as a game at home with the use of a webcam. The system records the evolution of the treatment and the performance of the exercise.
Rehabilitation service (SER) by CARTIF for Tratamiento 2.0 platform
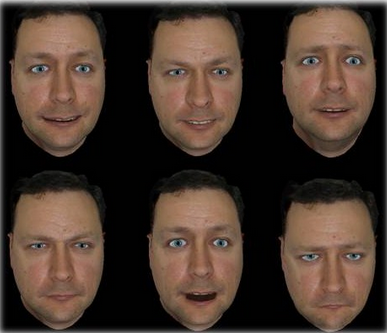
Emotional evaluation system developed by CARTIF. The system generates situations and emotions through an avatar of a person to identify them by people with schizophrenia. It can be used in diagnosis, treatment and evaluation of progress.
Emotional evaluation system developed by CARTIF
Education
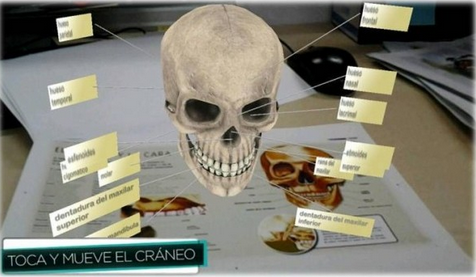
In this aspect, the AR provides a new channel that allows improving the learning providing other points of views on the knowledge. An example is the books that through mobile applications allow seeing parts of the anatomy in 3D.
Anatomy book with augmented reality
The use of these technologies is based on a series of techniques that make possible its use. Any advance in these techniques greatly improves the technologies. The main techniques used are:
Registration of information and monitoring: It is very important to position the user to be able to correctly locate the contents in their environment even if the user or objects move or even partially cover. This is done through visual marks such as bidis that are identified by the system and allows accurate placement of the contents.
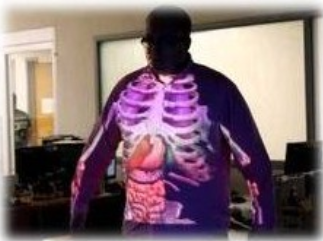
Display screens. It allows integration between the real and the virtual. The most striking technique is the use of head screens (smart glasses) that allows the user to see the physical world through the lens and superimpose graphic information in the user’s field of vision by reflecting it in their eyes. Other techniques are screen in hand (mobile or tablets) that capture the physical world with a camera and overlay graphic information on the video. Space projection uses digital projectors to display graphic information about physical objects.
El uso de estas tecnologías se sustenta en una serie de técnicas que hacen posible su utilización. Cualquier avance en estas técnicas mejora enormemente las tecnologías. Las principales técnicas usadas son:
Registration of information and monitoring. It is very important to position the user to be able to correctly locate the contents in their environment even if the user or objects move or even partially cover. This is done through visual marks such as bidis that are identified by the system and allows accurate placement of the contents.
Display screens. It allows integration between the real and the virtual. The most striking technique is the use of head screens (smart glasses) that allows the user to see the physical world through the lens and superimpose graphic information in the user’s field of vision by reflecting it in their eyes. Other techniques are screen in hand (mobile or tablets) that capture the physical world with a camera and overlay graphic information on the video. Space projection uses digital projectors to display graphic information about physical objects.Head screens
Screen in hand (mobile or tablets). Guidance System (STAR)
Space projection
In order to interact with these systems, typical interfaces such as touch screen, mouse, keyboard or more advanced and specific interfaces such as gloves, brain interfaces or simulation tools are used as surgical material …
As we have seen, AR and VR have promising potential for use in medical applications because it provides seamless integration of data visualization with the patient’s body. This allows for improved methods of medical diagnosis and treatment.
There are technological limitations especially on the screens and registration of data that make this technology have not yet a realistic clinical application in a regular medical environment, but the progress in several R&D projects and the interest shown by the researched ones is encouraging.
Finally, it is necessary to solve a great challenge that is often overlooked and is to improve the real usability of these systems, avoiding the sensory overload and making the viewing experience more controllable, simple, agile and transparent so that the only concern of the medical staff is the patient.
Technology is very present in our lives. Proof of this is the increasing use of computers, smartphones, tablets and video games. Technology helps us with daily tasks, provides entertainment and fun, but can also improve fields such as medicine and health by helping to understand concepts, forming and encouraging both patients and healthcare personnel.
Technologies such as virtual reality, augmented reality and mixed reality have been introduced in our lives mainly through video games and have a lot of potential for implementation in the world of health. Everybody knows about these concepts but we are going to comment these terms to avoid confusion.
The mixed reality (MR) consists of combining the virtual world and the real world, creating spaces where virtual objects interact with real people and vice versa. The degree of mixing between these two worlds gives rise to the concepts we know as augmented reality and virtual reality.
The augmented reality (AR) is a simplification of the mixed reality where the user is stimulated with virtual contents in real time.
Virtual reality (VR), however, consists of virtual iteration with virtual objects in a virtual environment.
The AR and MR technologies have a wide field of work in the medical field, such as the fusion of the 3D data of the medical examination with the patient’s view that allows improving the precision in the diagnoses. AR has a clear application in supporting surgery, while VR is more suitable for simulation without the actual patient. Any of these technologies can be used for the training of doctors and medical students, as they improve the situation and the spatial awareness of the practitioner. In addition, the patient can also be supported by a variety of applications through this technology focused on training, treatment, rehabilitation…
These technologies have been used for many years in different aspects of medicine. After the explication of these three reality types, my next post will be based on the application of them in the health field.
Few days ago, the European project LIFE DIOXDETECTOR was closed in CARTIF. The main objective was the application of a new analytical technique for the quantification of dioxins and furans, being this new technique, mainly, more sensitive and faster with respect to technical traditional.
Dioxins and furans are compounds that form part of a group of dangerous chemicals called Persistent Organic Pollutants (POPs).
When the word “dioxin” is heard, a certain alarm is created, and it is no wonder, because they are “worrying” compounds because of its high toxic potential as well as its persistence in organisms. The half-life of dioxins in an organism is between seven and ten years.
Big catastrophes such as, the serious accident in 1976 at a chemical factory in Seveso (Italy) or high concentrations of dioxins were found in poultry and eggs from Belgium in 1999 or market exit of tons of meat pork and pork products in late 2008 in Ireland, since amounts of dioxins were detected 200 times above the limit prescribed, among others…have been used to study the effects of long term dioxins and furans cause on health and the environment.
Dioxins and furans emission sources are mainly, solid waste incineration, industrial processes (paper mills, foundries, etc.) and road traffic, but also can also be generated naturally (forest fires, etc.).
And it is that although, the problem of dioxins and furans appear that it is so far, because it is possible that you do not live near an incinerator, due to the generalized presence of these compounds, all people have background exposure, which is not expected to affect human health. The effects on human health depend on the time of exposure to these pollutants.
These compounds can cause reproduction and development problems, affect the immune system, interfere with hormones, and in this way cause cancer.
In the environment, studies show that soil and vegetation near incinerators, can become contaminated by the release of dioxins and heavy metals at levels above normal background concentrations. The dioxin levels found in the soil and vegetation depend on the distance to the incinerator.
As cited above, solid waste incinerators are one of the main emissions sources of dioxins and furans. The European Directive for hazardous waste 2000/76, transposed into Spanish law in RD 653/2003, establishes as limit total emissions of dioxins and furans 0.1 ng/Nm3.
Undoubtedly, the most effective measures to prevent or reduce human exposure to these compounds are those taken at the root, i.e., in the own emission sources, with more stringent controls industrial processes in order to minimize the formation of dioxins and furans.
The analysis of these compounds is one of the most complicated in the world. The high toxicity of these compounds at very low concentrations, makes necessary the development of highly sensitive analytical techniques, as the technology proposed in the DIOXDETECTOR project, which is able to detect concentrations below the level of part per quadrillion (ppq).
It is clear that an improvement in air quality, it is quality of life. Just have to take a look at the latest news related to air quality: “Madrid exceeds the limits for nitrogen dioxide and active phase 2 of the protocol anti-pollution City” or “The poor air quality in Aviles forces to decree the pre-pollution alert”, among others, to realize the consequences that entails poor air quality in our daily lives.
You can think that the design of differentiable technology for menand technology for woman is not necessary. But, really specific wearables for women exist, especially for health topics. The others wearables, despite not being specific for woman, have a feminine designed due to some fashionable aspects.
I am going to mention several of these devices. Some of them are at the market, but others ones not yet, because they are pending of financing (almost always by crowdfunding), in order to going on with its development and coming out to the market. However, results are real for all them.
WEARABLES FOR WOMEN’S HEALTH
In relation with health topics, we find a big variety of devices focused on biological questions, such as control menstrual cycle or maternity and pregnancy aspects. For example:
– Leaf, a popular jewel due to its design, is developed to make fertility tracking. To keep track of monthly cycles. The technological advantages are its autonomy (six months) and capacity (dates for 14 days can be recorded without the connection to an app) – YONO Fertility Friend. This device is introduced in the ear and collects basal temperature overnight. Through an intelligent system, predicts and reports fertil days’ information. – The ReliefBan bracelet serves to avoid the morning sickness in pregnancy period. The operating philosophy is as of acupuncture. It consists of two electrodes that distract the nervous system through electrical impulses. The brain is distracted and the pain is blocked. – Milk sense is placed at breast, before and after feeding during lactation period. It uses alveoli changes for determinate the milk quantity that the baby needs.
WEARABLES FOR WOMEN BECAUSE OF ITS DESIGN
They are device that do not have a concrete function for women but the design is for them. Some examples
– Ombra works as every sportive device. The main difference is that its sensors are integrated in the brassiere. – Swarosvki offer us the Lumo Lift. It is a brooch with a sensor, which alerts us when our back position is not correct. – At the frontier, we have the Firs Sign forks. The pin detects possible assaults. It has a sudden movement detector. Immediately, it connects to the camera of our smartphone and alert to emergency services. Smartphone provides them the localization, also. – In addition, there are intelligent devices for solar protection, such as bracelets, towels, bikinis with UVA sensor, etc. These sensors, via RFIDs, send alerts to smartphone, depending on every skin type.
FASHION WEARABLES
Talking about decorative or fashion aspects, we have a big offer of wearables. It is said that the bet of important trademarks (such as Swarosky or L’Oreal) allows us to intuit that the fashion-technology fusion will have an important market of the near future.
Inside this group we have jewels with same or similar functions as the smartwatch:
– The Ringly ring is synchronized with smartphone for warning to alerts and calls through colour and vibrations. – The Hungary ring Omate, presented in gold, silver or precious stones. – The TagoArc bracelet is characterized by having an electronical ink covering. An associated app allows us to select the design of bracelet and change them when you want.
If we talk about fashion complements, taking out jewels, we have a wonderful offer from the more practice devices, (such as intelligent handbags that allow to charge phone), to the most ostentatious.
I want to highlight the experiments that Ezara and Tuba Cintel are designed, with Intel enterprise; the “dress of butterflies”. This dress remembers the fiction models of Katniss Everden at “The Hunger Games”
Before introduce our vision of interoperability of social-health system, it is needed to understand that interoperability is the ability of two or more systems or components to exchange information and to use the information that has been exchanged. As organizations incorporate applications / different computer systems, they generate what is known as “islands” of information, which end up generating gaps in services as well as inefficiency bags. Interoperability is the design and construction of bridges between the islands of information.
The Social-Health system in Spain, as well in Europe, consists on a large number of organizations, public and private entities: healthcare systems, social agencies, patient associations, services companies, nursing home, etc. Each of these organizations provides the services we need to develop our lives and those of our loved ones, in a comfortable way taking into account parameters of quality and efficiency.
One doubt that often arises in meetings with different partners is the real need to develop an interoperability framework for the social-health system. The intuitive answer to this approach is like building roads, tunnels and bridges, without prior planning. Does anyone find reasonable such approach?
However, in general, when organizations develop strategic plans for information technology (IT) tend to look inward, focusing mainly on achieving their own goals (an apparently optimal island). Further progress in this direction certainly hinders the 360º approach (continuity in health and social services). The challenge is to go beyond the internal problems and look outside. It needs to take advantage of the information generated by all organizations, so that, they can share and use the data, to generate new knowledge.
So we must begin to understand and to harmonize the needs of users and organizations from a scientific and technical systematic view. Once the doubt of working on a strategic framework of interoperability is clarified, the following question emerges: why is it necessary to base a local or regional strategy on international standards? Why is it not possible to make a local or an ad-hoc approach?
One possible approach to this question is associated with the sustainability of the work and to take advantage of an accumulation of knowledge (not reinventing the wheel). Therefore, in order to advance into a strategy of interoperability between of social and health information systems, it is critical to be based on international interoperability standards. These standards are promoted by Standards Development Organizations (SDOs) with the need to work actively through scientific and technical committees that contributes to the necessary evolution of standards forums.
Thanks to the experience of CARTIF, participating in different SDOs, as well as in the Cluster SIVI (Cluster of Innovative Solutions for Independent Living) and the EIP AHA (European Innovation Partnership on Active and Healthy Ageing), we conclude that a strategy to develop a framework of interoperability in social-health system, could open the door to cooperation between organizations in different fields, who want to be an active part of the social and health services. The beneficiaries of this cooperation are all users of the system (all of us!!), because it could be optimized and rationalized the use of resources, something that is extremely important to ensure the sustainability of the social-health system. On the other hand, this would increase the transparency and competitiveness of technology to develop new solutions that can be extended in a simpler way. Finally, we are convinced that the approach of advancing within a framework of interoperability in the social-health system will help develop new products in emerging technology SMEs. Solutions that succeeding locally, will be able to scale their solutions to a global market in a simpler way.
The Abdominal Aorta Aneurysm (AAA) has been recognized as a major health problem in the last decade. The statistics associated with this condition are of great concern and, as recorded in most of the studies found in scientific literature, it is expected that its impact will increase in the next years mainly due to the increase in life expectancy of the population. The rupture of abdominal aortic aneurysms represents a major clinical event because of its high mortality rate.
According to Dr. Felix Nieto comments in his previous post, currently the indicators used to determine the treatment of patients with aneurysms are the maximum transverse diameter and the growth rate that can be considered insufficient; they do not have a physically grounded theoretical basis. Because of this limitation, in recent years research has been basically aimed at improving understanding of the phenomena associated with the emergence and evolution of this disease, in order to determine whether other variables could be predictive of rupture.
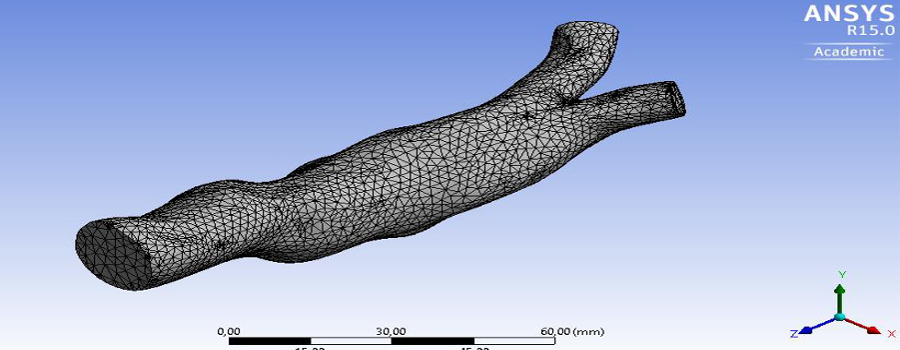
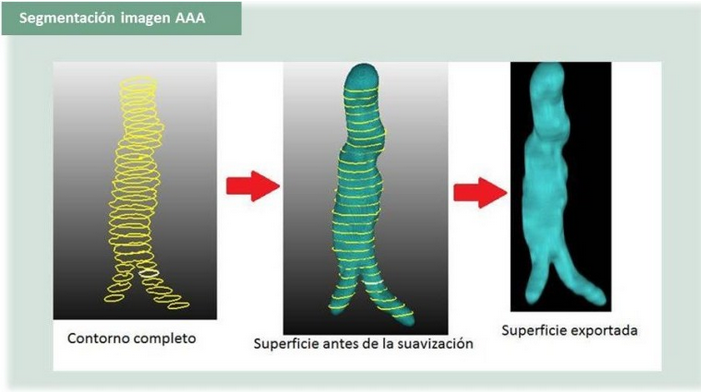
One of the major constraints in obtaining accurate results in modeling vascular diseases is the use of a realistic computational domain, which is closer to be possible due to technological advances in equipment for conducting tomography computed axial (CT), magnetic resonance imaging (MRI) and the development of CAD techniques, which has advanced significantly in the detailed extraction, in vivo, of anatomical structures.
CARTIF team is working on automated conversion of 2D set of images obtained by CT in a realistic 3D model that constitutes the geometric domain of integration into the AAA simulation by finite element techniques
The activity related to medical imaging AAA has been the key to one of the issues recently treated in CARTIF, called the study of the influence of geometric parameters on the rate of rupture of AAA, the work is particularly focused on iliac angle.
In the first phase they were carried out fluid dynamics and structural simulations to calculate the Rupture Potential Index (IPR) of several cases of patients affected by AAA
The results show that the values of the iliac angle (α) are related to other geometric parameters such as the eccentricity of AAA, which together can characterize the IPR.
The next step would confirm this trend over a larger database of patients with AAA, being essential as now, the good cooperation with HCUV (University Clinical Hospital of Valladolid).
For the simplicity of obtaining these parameters by the specialist through the TAC, the results of this research could be a very effective tool for the surgeon when making the decision to submit or not the patient to a surgical repair procedure.









{kind=link}